MEDITERRANEAN DIET – DOES THE GI MATTER?


The health benefits of a Mediterranean diet (Med-diet) are simply undeniable. But what exactly do we mean by a Med-diet and does it matter if the carbohydrates that are consumed as part of it are low or high glycemic index (GI)?
What exactly is the Mediterranean diet?
The traditional Mediterranean diet was originally found in the olive growing areas of Crete, Greece and Southern Italy in the late 1950s. In his 7-countries study, Ancel Keyes noted that coronary heart disease was uncommon in this part of the world in comparison to other nations at the time. He ascribed the difference to the amount and nature of the fat and its effect on blood cholesterol.
A Med-diet is not defined by any one ingredient – it’s not just the abundant use of olive oil – indeed, the oil could be any of a number of oils – and it’s not just the wine either (sorry!). There’s a useful food pyramid published by Oldways (1) that describes it well:
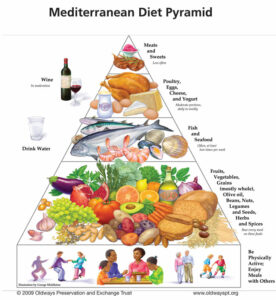
According to Jorde Salas-Salvado, the major characteristics are:
- High consumption of cereals, legumes, nuts, vegetables and fruits
- Relatively high fat intake, mostly provided by olive oil
- Moderate to high fish intake
- Poultry and dairy products consumed in moderate to small amounts
- Low consumption of red meats and meat products
- Moderate alcohol intake, usually in the form of red wine
In a review of the scientific literature (2), a Med-diet was found to contain up to 9 serves of vegetables, 2 serves of fruit, up to 13 serves of cereals and 8 serves of olive oil. In macronutrient terms, that’s ~37% of energy as fat (and that’s a lot of fat) but only 9% saturated fat. Red meat and sweets are eaten occasionally.
What are the health benefits?
The evidence supporting a Med-diet for good health includes two landmark studies in nutrition – the Lyon Heart Study published in 1994 and the PREDIMED study published in 2018.
With so much fat, you would be forgiven for thinking it’s bad for body weight. But a study published in the New England Journal of Medicine in 2008 (3) reported higher weight loss on a Med-diet than a low-fat diet. Furthermore, among those with diabetes, changes in plasma glucose and insulin were more favourable among those assigned to the Med-diet. A third group, made up of those instructed to follow a low carb diet, lost more weight to begin with, but weight regain was common. Those assigned to the Med-diet, lost weight and kept it off for at least 2 years.
Recently, Gabriele Riccardi and colleagues in Italy, Sweden and the United States conducted a 12-week randomised controlled trial to determine if a Med-diet incorporating low GI foods was superior to a standard Med-diet (4). All participants were advised to consume the same amount of carbohydrate (270 g/day) and fibre (35 g/day). One half of the carbohydrate was the same for both the high and low GI groups, including fruits and vegetables. The other half (135 g/day) came from foods with GI values less than 55 (the low GI group) or foods with a GI > 70 (the high GI group). The authors reported that post-meal glucose fluctuations were 35% higher after high GI meals and worsened over time, while indices of glycemic variability were reduced in the low GI arm. Changes in glycated hemoglobin (HbA1c) were similar in both groups.
Glycated hemoglobin is currently the gold standard for assessment of overall glycemic control because it predicts the risk of developing complications in people with diabetes. However, fluctuations in blood glucose are now known to be associated with increased risk, independent of glycated hemoglobin. The risks include lower sense of well-being and quality of life, higher inflammation and oxidative stress, factors known to be linked to cardiovascular disease. The ability to assess glycemic variability with continuous glucose monitoring devices gives us a window into minute-by-minute metabolism that we didn’t have in the past.
A low GI Med-diet may also be the best diet for people with fatty liver disease, specifically non-alcoholic fatty liver disease (NAFLD). This disease is currently the most common form of liver disease worldwide affecting all ages and ethnic groups, even in young people. Osella and colleagues from Southern Italy assessed changes in NAFLD score using ultrasonography in a randomised controlled trial lasting 6 months (5). The low GI Med-diet was found to decrease the NAFLD score within a short space in time.
So…. my take-home messages from recent research is that it’s possible to make a Med-diet even healthier by:
- Using wholegrain, low GI cereals
- Using extra-virgin olive oil, canola oil or other oil rich in alpha-linolenic acid
- Increasing the consumption of fatty fish
- Eating nuts daily
- Reducing sodium (salt) intake
- Moderating consumption of wine with meals
Read more:
- Oldways Mediterranean Diet Pyramid
- Davis and colleagues. Definition of the Mediterranean Diet; A Literature Review. Nutrients, 2015.
- Shai and colleagues. Dietary Intervention Randomized Controlled Trial (DIRECT) Group. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N Engl J Med. 2008
- Bergia and colleagues. Differential Glycemic Effects of Low- versus High-Glycemic Index Mediterranean-Style Eating Patterns in Adults at Risk for Type 2 Diabetes: The MEDGI-Carb Randomized Controlled Trial. Nutrients 2022
- Misciagna and colleagues. Effect of a Low Glycemic Index Mediterranean Diet on Non-Alcoholic Fatty Liver Disease. A Randomized Controlled Clinical Trial. J Nutr Health Aging. 2017
Professor Jennie Brand-Miller holds a Personal Chair in Human Nutrition in the Charles Perkins Centre and the School of Life and Environmental Sciences, at the University of Sydney. She is recognised around the world for her work on carbohydrates and the glycemic index (or GI) of foods, with over 300 scientific publications. Her books about the glycemic index have been bestsellers and made the GI a household word.

Latest Blog Post List




